
Osteoporosis & Oral Health
Osteoporosis is a condition that weakens bones and makes them more prone to fracture. Estimated to affect about 10 million Americans at present, it causes some 2 million fractures each year — and as our population ages, these numbers are expected to increase. Osteoporosis can affect any part of the body — including the jawbone that supports the teeth.
This may be of particular concern if you are considering certain dental procedures — for example, getting dental implants to replace missing teeth. Implants are today’s gold standard for tooth replacement, because they look and function so much like real teeth. But their success depends on a process known as osseointegration, by which they fuse to living bone in the jaw. For this to occur, that bone must be relatively healthy; yet osteoporosis — and certain medications used to treat it — may affect your oral health.
Bone: An Ever-Changing Tissue
The living bone tissue in the body isn’t like the dry, white skeleton you may have seen in a doctor’s office or on TV. It is constantly being remodeled by two natural processes: resorption, in which the body removes and breaks down old, damaged bone; and bone formation, where the removed material is replaced by new, healthy bone. In an ideal situation, both processes happen at an equal rate; osteoporosis, however, tips the balance toward resorption, weakening the bone structure.
A class of drugs called bisphosphonates (whose brand names include Fosamax, Boniva, Reclast and Prolia) can inhibit resorption and help bring the two processes back into balance. But for reasons that aren’t fully understood, these medications sometimes have a different effect on the bones of the jaw. In rare cases, long-term bisphosphonate users experience osteonecrosis of the jaw (ONJ), a condition in which isolated areas of jawbone lose their vitality and die. If you are a candidate for oral surgery, tooth extraction or implant placement, it’s important to consider the possible effect of bisphosphonate use before you have this type of procedure.
Taking Medication
Over 90 percent of the people who suffer from bisphosphonate-associated ONJ received high doses of the medication intravenously — often for cancer treatment. Only a small percentage of those who take the drug orally are likely to develop this condition. So generally speaking, if you have osteoporosis or are at high risk of bone fractures, the benefit of taking these medications far outweighs the risk.
But if you are about to begin therapy with high doses of bisphosphonates, it’s ideal to have a dental exam and resolve any oral disease before beginning the medication. Likewise, while you’re receiving the medication, it’s best to avoid invasive dental treatments if possible. However, since untreated oral disease may cause serious health problems, be sure to discuss the situation with all members of your medical team before making treatment decisions.
Most people who take oral bisphosphonates for osteoporosis won’t have to postpone or avoid dental procedures, because they have little risk of developing ONJ. In the case of dental implant placement, the decision to proceed is made on an individual basis, after a thorough examination of the quality and quantity of tooth-supporting bone in the jaw. The presence of osteoporosis may influence the type of implants used, and the amount of healing time needed to complete the osseointegration process.
No matter what dental procedures you are considering, it is vital to keep us informed about any medical conditions you have, and any drugs you may be taking — both prescription and non-prescription.
Preventing Osteoporosis
There are several ways you can help prevent osteoporosis. For a start, make sure you’re getting enough calcium and vitamin D. It also helps to decrease your caffeine and alcohol intake, and quit smoking. Weight-bearing exercise — physical activities that force you to work against gravity, like walking, jogging or weight training — can bring a host of benefits. And don’t forget your regular visits to the dental office. Your dental professionals don’t just help you to maintain good oral health — we encourage you to keep up your overall health as well.

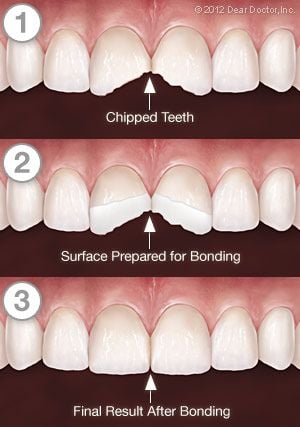 Firmly anchored in your jaw and protected by an outer coating of tough enamel, your teeth are remarkably strong — yet it’s still possible for them to chip, crack, or even break. In fact, there is some evidence that today, our teeth are developing cracks at a record rate. This may be due to the fact that people are living longer (giving teeth more time to accumulate damage), or that our stress levels are increasing (which may cause teeth clenching and grinding).
Firmly anchored in your jaw and protected by an outer coating of tough enamel, your teeth are remarkably strong — yet it’s still possible for them to chip, crack, or even break. In fact, there is some evidence that today, our teeth are developing cracks at a record rate. This may be due to the fact that people are living longer (giving teeth more time to accumulate damage), or that our stress levels are increasing (which may cause teeth clenching and grinding).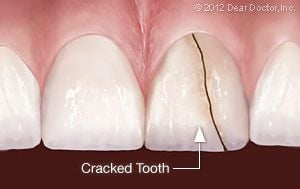 This type of crack often starts at the chewing surface and extends toward the roots — but may it also begin in the root and continue toward the crown. Either way, it doesn’t completely separate the tooth into two parts. Depending on the extent of the fracture, you may feel only minor discomfort that occurs in response to temperature changes (with hot or cold beverages, for example); or, it may produce sharp pain when you chew. In any case, you shouldn’t ignore the symptoms, because cracked teeth require dental treatment quickly to keep them from progressing further. If the cracks continue to progress, tooth extraction may become necessary.
This type of crack often starts at the chewing surface and extends toward the roots — but may it also begin in the root and continue toward the crown. Either way, it doesn’t completely separate the tooth into two parts. Depending on the extent of the fracture, you may feel only minor discomfort that occurs in response to temperature changes (with hot or cold beverages, for example); or, it may produce sharp pain when you chew. In any case, you shouldn’t ignore the symptoms, because cracked teeth require dental treatment quickly to keep them from progressing further. If the cracks continue to progress, tooth extraction may become necessary.
 This specially designed toothbrush (sometimes called an interproximal brush or proxabrush) can be successfully utilized to clean the small gaps between teeth, as well as the gums and the areas around braces, wires, or other dental appliances. Because it has a handle not unlike a standard toothbrush, many people with limited dexterity find it easy to use. Plus, numerous clinical studies have demonstrated its effectiveness at reducing plaque and controlling gingivitis (gum inflammation).
This specially designed toothbrush (sometimes called an interproximal brush or proxabrush) can be successfully utilized to clean the small gaps between teeth, as well as the gums and the areas around braces, wires, or other dental appliances. Because it has a handle not unlike a standard toothbrush, many people with limited dexterity find it easy to use. Plus, numerous clinical studies have demonstrated its effectiveness at reducing plaque and controlling gingivitis (gum inflammation).


 There are many elements that make up an ideal smile; bright, healthy-looking teeth immediately come to mind. But the gum tissue that surrounds and supports those teeth also plays a big role in how appealing your smile will look.
There are many elements that make up an ideal smile; bright, healthy-looking teeth immediately come to mind. But the gum tissue that surrounds and supports those teeth also plays a big role in how appealing your smile will look.
 One is severe crossbite, a condition where the upper teeth close inside the lower teeth. To treat this problem, a device called a palatal expander can be used, which gradually and painlessly widens the upper jaw; it’s especially effective when the jaw itself hasn’t fully developed. If one waits too long, a more complicated treatment — or even oral surgery — might be required to correct the problem.
One is severe crossbite, a condition where the upper teeth close inside the lower teeth. To treat this problem, a device called a palatal expander can be used, which gradually and painlessly widens the upper jaw; it’s especially effective when the jaw itself hasn’t fully developed. If one waits too long, a more complicated treatment — or even oral surgery — might be required to correct the problem. Another condition that may benefit from early treatment is severe crowding. This occurs when the jaws are too small to accommodate all of the permanent teeth. Either palatal expansion or tooth extraction may be recommended at this point, to help the adult teeth erupt (emerge from below the gums) properly. Even if braces are required later, the treatment time will likely be shorter and less complicated.
Another condition that may benefit from early treatment is severe crowding. This occurs when the jaws are too small to accommodate all of the permanent teeth. Either palatal expansion or tooth extraction may be recommended at this point, to help the adult teeth erupt (emerge from below the gums) properly. Even if braces are required later, the treatment time will likely be shorter and less complicated. Early intervention may also be helpful in resolving several other problems. Protruding teeth, especially in front, can be prone to chipping and fractures; they may also lead to problems with a child’s self-image. A severe underbite, caused by the lower jaw growing much larger than the upper jaw, can result in serious bite problems. Orthodontic appliances, including braces and headgear, can be successfully used to correct these problems at this stage, when the child’s development is in full swing, thereby increasing the chances that surgery can be avoided.
Early intervention may also be helpful in resolving several other problems. Protruding teeth, especially in front, can be prone to chipping and fractures; they may also lead to problems with a child’s self-image. A severe underbite, caused by the lower jaw growing much larger than the upper jaw, can result in serious bite problems. Orthodontic appliances, including braces and headgear, can be successfully used to correct these problems at this stage, when the child’s development is in full swing, thereby increasing the chances that surgery can be avoided.



